Price observed that peoples living on their native diets exhibited no cases of TB, in spite of constant exposure to smoke from wood or peat in their dwellings, but that the disease was rampant in those born to parents who consumed the “displacing foods of modern commerce” and had narrow faces with crowded and crooked teeth. He believed that poor diet in utero and during the period of growth resulted not only in weak facial development, but also a weakness in the lungs, making the offspring especially vulnerable to lung tissue breakdown, a hallmark of the disease.
Both Hippocrates and Weston Price recognized the role of diet in the treatment of TB. In the era of Hippocrates, treatment took place in temples where patients received plentiful and good food, especially milk, particularly asses’ milk, along with fresh air and sea breezes. The Greek physician Galen (129 – 216 AD) and other physicians of his time recommended fresh air, milk, particularly human breast milk, eating wolf livers and drinking elephant urine. Pedacius Dioscorides, a Greek army surgeon in the service of Nero (54-68 CE), recommended “warming drugs” such as animal fats; and Tertullian (160-225 CE) recommended butter boiled with honey.
Others fingered toxins as the culprit. In the early 1800s, Thomas Willis speculated that TB was caused by consumption of sugar, causing an acidity of the blood.
TB became epidemic during the industrial revolution of the 18th and 19th centuries, with observers linking the disease to social conditions of the time–poverty, malnutrition and overcrowding—in the working classes. In 1838 and 1839 in England between a quarter and a third of those who died of TB were tradesmen and laborers compared to a sixth of “gentlemen.”
In summary, early observers linked TB with injury, malnutrition and toxins. The first to propose contagion as the cause was Girolamo Fracastoro, who in his 1546 work De contagion, proposed that “phthisis” (the word used in the 16th century), was transmitted by an invisible virus, which he believed was contagious through direct contact with the discharged fluids of the infected.
By the 18th century many Italian physicians had come to believe that phthisis was infectious, and they avoided doing autopsies on patients who had died from phthisis to protect themselves and their students. But British and American physicians of the time disagreed, many believing that the disease was hereditary or, like Weston Price, ascribing the illness to constitutional weakness.
Conventional medicine gives credit to German physician Robert Koch for revealing that “TB is caused by an infectious agent.” March 24 1882 was the date of his famous report to the Physiological Society of Berlin. Koch cited the work of researchers who induced tuberculosis in animals by injecting them with tubercule matter from animals which had died of the disease, especially the experiments of Jean Antoine Villemin, who seemed to demonstrate in 1869 that the disease was contagious by injecting tuberculous matter from human cadavers into laboratory rabbits, which then became infected. Villemin, a French military surgeon, observed that soldiers stationed for long times in barracks were more likely to have phthisis than soldiers in the field, and that healthy army recruits from the country often became consumptive within a year or two of taking up their posts.
In his report, Koch proceeded to describe how he identified the tuberculosis bacillis by staining tuberculous matter with a blue dye, growing the organism on a preparation of ox blood, and then, using disinfectants at the site of the inoculation, injecting animals with the culture. With few exceptions, the animals developed granulomas containing the bacilli at the site of the injection and in nearby organs, and eventually died.
Key to Koch’s arguments were the experiments of Austrian scientist Franz Tappeiner, who “has been successful with inhalation.” In an 1877 paper, Tappeiner noted “the repeated observation that very healthy girls from a healthy family became phthisic themselves after prolonged care of a phthisic patient and died quickly.” This strengthened Tappeiner’s suspicion that TB was a contagious disease “caused by inhalation of phthisic sputum, which was atomized by coughing in the air,” even though experimental methods available at the time (inoculation, feeding and forced tracheal introduction) had failed to provide conclusive results.
In his presentation, Koch then proceeded to describe experiments in which he inoculated material from scrofulous glands or fungal masses from joints in which no tubercle bacilli could be found. “In these cases, not a single animal became sick, while the animals inoculated with bacilli-containing material, always showed an extensive infection with tuberculosis after four weeks.”
He concluded: “All of these facts taken together lead to the conclusion that the bacilli which are present in the tuberculous substances not only accompany the tuberculosis process, but are the cause of it. In the bacillus we have, therefore, the actual tubercle virus [poison].”
Koch’s report was published as a letter in the Times, April 22, 1882 and subsequently in the New York Times, the New York Tribune and other newspapers from around the world, launching the germ theory into public consciousness. Koch won the Nobel Prize in 1905.
The case for the infectious nature of TB seemed irrefutable. . . yet many are still skeptical, still asking questions. For example, how could “inhalation of phthisic sputum, which was atomized by coughing in the air,” cause TB when forced tracheal introduction of tuberculous material had failed to provide conclusive results. If TB is spread by coughing, how is it that any TB caretakers survive? How did Florence Nightingale or any of her nurses survive the Crimean War, for example? If exposure to coughing patients is so deadly, any assignment of medical personnel to a TB ward would be a death sentence.
The skeptic who introduced me to a different way of thinking about TB was the late Mark Purdey, known for his disagreement with government pronouncements about the cause of mad cow disease. When some of his dairy cows tested positive to TB, he began to ask questions. Why were so many cows on farms in the area suddenly coming up positive? He noted that for several years, tight finances had prevented farmers from applying lime to their fields, resulting in more acidic soils. “The relevant issue in respect of TB infection and soil acidity hinges on the fact that acidification of the topsoil leads to an excessive accumulation of available iron, particularly in regions where soil iron is naturally elevated and rainfall is high.”
Today, we know a lot more about mycobacteria—the species associated with TB—than nineteenth century researchers did. Like so many bacteria considered “pathogens,” mycobacteria are iron-loving organisms, which proliferate in environments of excess iron—thus Koch was able to cultivate the bacillus on iron-rich ox blood, and sometimes on iron-rich meat, but not on other substances. We also know that the TB bacillus is ubiquitous, always there in the soil and most likely in small amounts in animals and human beings. Up to nine out of ten people who test positive for the TB bacillus exhibit no signs of the disease—a condition called “latent TB.”
Let us consider iron oxide–a poison given off by iron that has been heated. Since the beginning of metallurgy, humans have suffered exposure to iron oxide—men working with iron, of course, but also those exposed to heated iron cookware in enclosed spaces. This can explain the occasional evidence of TB in the remains of pre-industrial peoples.
With the industrial revolution that exposure increased—in iron mines, in foundries that worked iron for all the new machinery, in ships with their iron boilers, in railway workers exposed to steam from cast iron boilers, from dense pollution in areas where the preferred fuel was certain types of iron-rich coal—iron is the most predominant metal in coal fly ash–and especially in war. Iron canons, iron gun barrels, iron hand grenades and iron cookware for feeding the troops all produced iron oxide; in trench warfare, the heavy pollutant would fall into the trenches and linger. Solders living in these trenches suffered massively from TB.
In 1790, a new invention not only increased exposure to iron oxide but also brought it into the drawing room: the cast iron stove.
 With large surface area, the cast iron stove can release large amounts of iron oxide, to which not only the cooks and maids in unventilated basements were exposed, but also madame and monsieur enjoying the comfort of a warm room upstairs, as the moist heat rose through iron piping. Or, they had a cast iron parlor stove dedicated to heating the living areas. We had just such an arrangement in our farm house—a cast iron stove in the entry way with rusty iron piping to take the heat upstairs. Fortunately for the previous owners, the stove remained largely unused after the installation of radiators—also made of cast iron, but not operated at such hot temperatures as cast iron stoves, and often painted, a practice that would reduce the off-gassing of iron fumes.
With large surface area, the cast iron stove can release large amounts of iron oxide, to which not only the cooks and maids in unventilated basements were exposed, but also madame and monsieur enjoying the comfort of a warm room upstairs, as the moist heat rose through iron piping. Or, they had a cast iron parlor stove dedicated to heating the living areas. We had just such an arrangement in our farm house—a cast iron stove in the entry way with rusty iron piping to take the heat upstairs. Fortunately for the previous owners, the stove remained largely unused after the installation of radiators—also made of cast iron, but not operated at such hot temperatures as cast iron stoves, and often painted, a practice that would reduce the off-gassing of iron fumes.
During the industrial revolution, crowding and poverty in the cities would have greatly increased exposure to iron oxide—whether from pollution, from a cooking pot over a coal fire in crowded quarters, or from a cast iron stove in an unventilated room. If a TB patient lay in bed near a cast iron stove for warmth, the care-taker as well as the patient would have breathed in iron oxide day and night.
Treatment for TB usually involved traveling to the countryside in the summer for fresh air and sunlight—eliminating exposure to iron oxide for a few months. Most protocols involved consuming raw milk—the lactoferrin in raw milk helps sequester iron and reduces the TB symptoms. The therapy often involved consumption of vitamin A-rich liver or butter—vitamin A is critical to healthy lung function and protection against heavy metals. The patients usually improved, but then regressed with renewed exposure to iron oxide when they returned to the cities in the Fall. Such was the plight of poor Violetta, the heroine of Verdi’s opera La Traviata. She develops TB while living a dissolute life in Paris, then recovers during her happy time with Alfredo while living in the countryside, then succumbs after returning broken hearted to the ornate parlor stoves of Paris—the stress of grief can rapidly use up protective vitamin A stores.
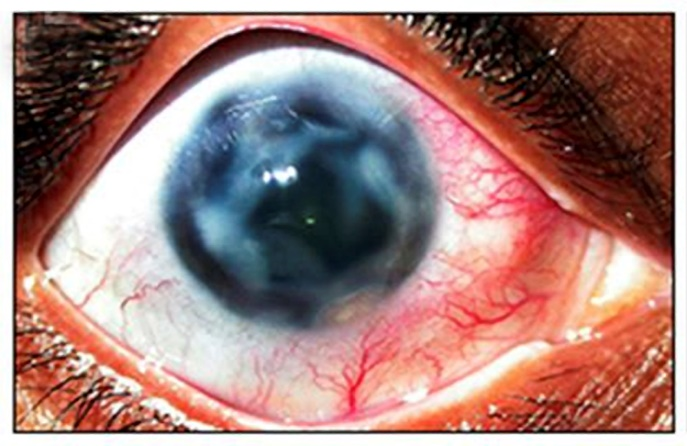
Iron poisoning is called siderosis, and its symptoms are the same as those of TB—cough and trouble breathing, of course, and sometimes coughing up blood. The characteristic miliary (millet seed-like) lesions of TB are not exclusive to the disease, but occur in other diseases, including siderosis. Siderosis can affect other organs besides the lungs—as does TB. One striking similarity is the darkening of the eyes, which occasionally occurs in both siderosis and TB.

Let’s return to Koch’s experiment. He induced lesions and found the TB bacillus in them by injecting the animals with a culture of TB bacillus grown on iron-rich blood. While he could claim that he had isolated the organism—in other words, there were no other types of bacteria in the culture—no culture is “pure,” meaning devoid of other substances. The culture would have been contaminated with iron, of course, and possibly contain toxins produced in the preparation of the ox-serum culture (which was heated several times, a process that can denature the many delicate substances in blood). And finally, the site of the injection was treated with an antiseptic, probably carbolic acid. In other words, there were certainly harmful substances, especially iron, in the injection, and granulomas—interpreted as TB—were the logical result.
When Koch injected animals with material from scrofulous glands or fungal masses, no lesions appeared—but these were not cultured on iron-rich blood that had been heated several times.
The key test is whether TB can be produced in the lungs by exposure to the TB bacillus in the air. For this he relied on the earlier experiment of Tappeiner, so it pays to look at it more closely. To prove contagion, Tappeiner purchased three dogs and kept them in a dog stall near a window and a door, “which was closed on all sides and connected to the air only at the front through a lattice-like open door at the top.” Tappeiner obtained sputa from a “phthisical afflicted locksmith.” He ground a tablespoon of this in a porcelain mortar with distilled water and put it in a “steam atomizer from Stiefenhofer.” He placed the atomizer in front of the kennel and allowed the nebulized liquid into the air of the kennel twice a day, for one to one and one-half hours. The upper lattice opening was hung with oil cloth “to better concentrate the dust.”
At the same time, Tappeiner mixed ground up sputum into the feed of two other dogs “to try whether absorption from the intestinal tract could also produce tuberculosis.” Tappeiner observed that all five experimental dogs appeared to be quite healthy, exhibited neither coughing nor diarrhea, ate with the best of appetites, and were lively and alert, without any sign of illness save for slight emaciation or lack of growth.’
Autopsies on the test animals performed after three weeks (on one inhalation dog) and six weeks (on the other four dogs) revealed small lesions (called miliary tuberculosis because the lesions resembled millet seeds) in the lungs, kidneys, liver and spleen, and in the feed dogs also of the intestinal tract. So while forced tracheal introduction of tuberculous matter failed to demonstrate contagion, a tiny amount of aerosolized sputum on a jet of steam did the trick.
I have been unable to locate a picture of a “steam atomizer from Stiefenhofer” but all the atomizing devices of the era were made with iron and brass, such as this example from 1875.

Heated brass can also give off iron fumes, as well as arsenic fumes, a double whammy. So did a tiny amount of bacillus from the lungs of TB patients induce lesions in the animals, or was it iron (and possibly arsenic) fumes in the steam?
The key question, not answered in Tappeiner’s report, concerns the two feed dogs—they were in a different stall, but were they in the same room as the three inhalation dogs? If so, they would also be subject to the steam and thus do not represent a real control.
Germ theory dictates the current treatment for TB—antibiotics and vaccinations—which health officials claim have successfully reduced the death rate from this terrible disease.
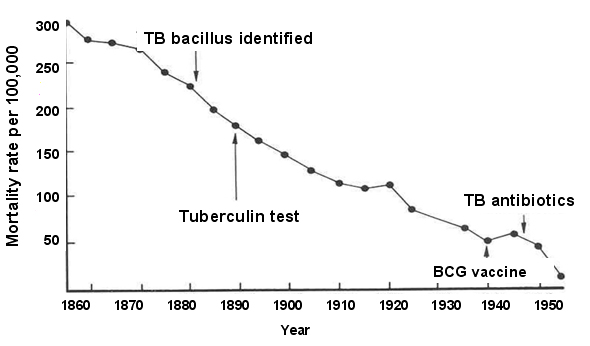
But note that mortality from TB was already falling, long before these interventions. As stainless steel and aluminum gradually replaced cast iron in stoves, furnaces and industrial equipment, household exposure to iron oxide gradually declined.
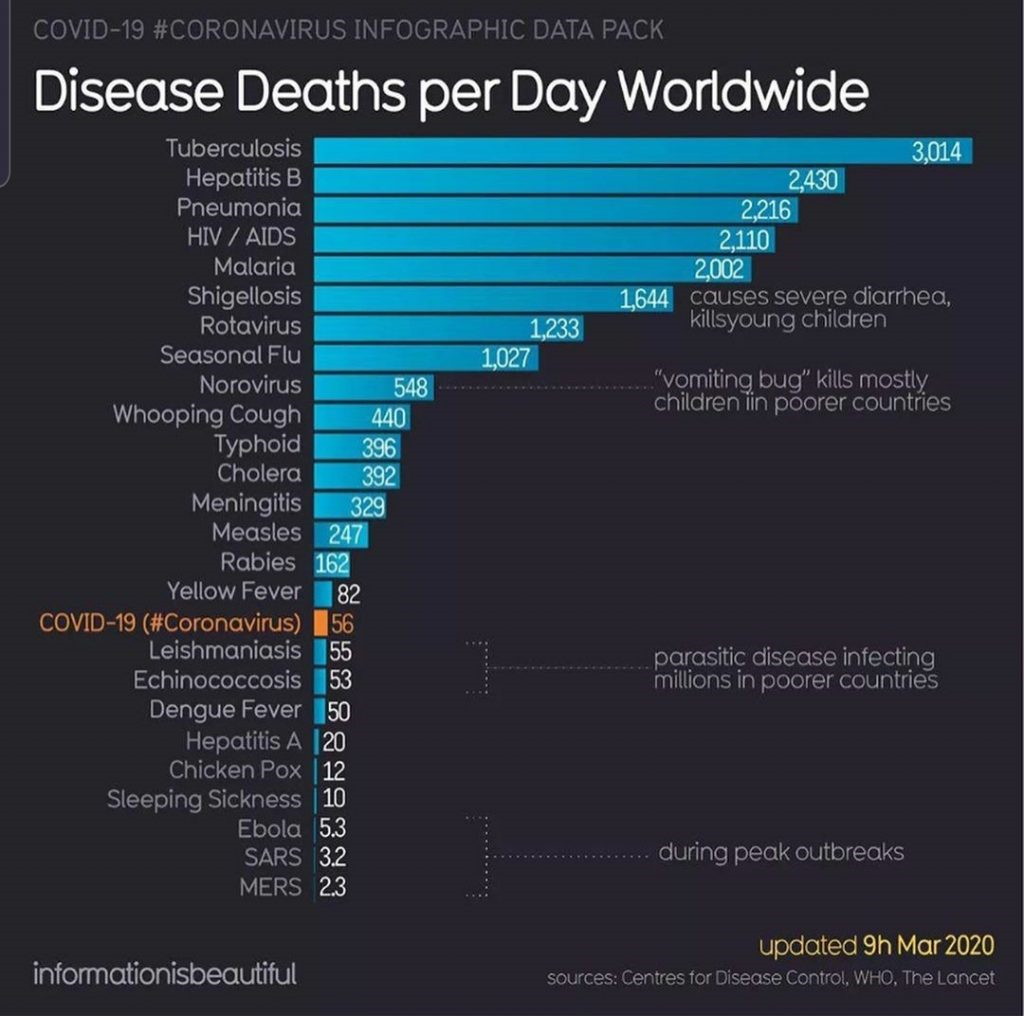
That does not mean we have solved the problem of TB. TB is still the world’s number one killer, with over 3000 deaths per day attributed to the disease.
These TB deaths occur mainly in the Third World where cast iron stoves and cookware (pots and griddles) are still widely used, often in unventilated hovels; iron mining and iron works are also common, typically with little concern for safety; coal is still used in powerplants and domestic settings in these areas.
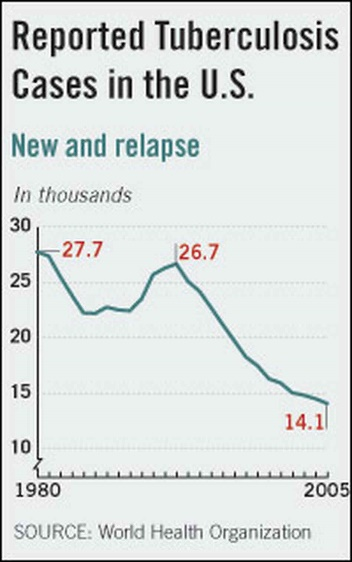
Even in the U.S., TB remains a problem.
Maybe we have failed to solve the mystery of TB because we are looking in the wrong place. Could it be that the bacillus associated with the disease is not the cause, but actually the therapy? Could it be that excess iron in the tissues calls on these ubiquitous critters to serve as a clean-up crew? Could be that Florence Nightingale—a mere nurse!—was the one who got it right in fingering noxious gases, and that the effects of this poison are exacerbated by poor nutrition and pre-natal injury?
Likewise, we will not solve the Covid problem if we are looking in the wrong place, if we blame continuing outbreaks—even in the vaccinated–on new virus variants until we run out of Greek letters. My colleague Tom Cowan and I are not alone in proposing microwave radiation poisoning from Wi-Fi and 5G as a major cause of this mysterious illness. The epidemiology fits, the biology fits. The solution is not vaccines and anti-virals, but the hard, unglamorous work of cleaning up our houses, our workplaces, our hospitals and our towns–and eating protective food– so that we can live safely with this new technology.
To read more about another germ theory charlatan, Louis Pasteur, see my post Anthrax, Arsenic and Old Lace
UPDATE: Guess what! In homeopathy iron and arsenic (Ferrous and Arsenicum) in potentized form (very diluted and succussed) are indicated for tuberculosis. The idea in homeopathy is that something in large quantities that would make someone sick, would in potentized form make one well. Just another indication that exposure to fumes of iron, and possibly to arsenic, is the cause of TB.
Much thanks to Tamara Romaine for her translation of the Tappeiner article from German into English.
The Weston A. Price Foundation is your source for accurate information on nutrition and health. Your membership supports the Foundation’s important work.
So should we get rid of our cast iron pans and what would be an acceptable alternative.
Was wondering the same since thats mostly what i cook in.
I have the same question as I was told those are the best for cooking
As far as I know, cast iron, properly seasoned with saturated fats, is completely save if used for frying. I’d never advise anyone to use cast iron for soups or acidic foods like tomato sauce. For such foods, I’d recommend glass ceramic or anything with an enamel coating.
Unless you live in a hovel, no ventilation, in toxic neighborhoods spewing out noxious gases, ur fine using ur cast iron and wood stoves.
Well seasoned cast iron pans used with an extraction fan to pull out the fumes are fine–I use cast iron myself.
Best,
Sally
Thanks Sally for your expertise on this
Hmmm.
Another reason that donating blood (lowering bodily concentration of iron) is a good idea?
Instead of giving blood, it might be better to lower the iron levels in the body by overnight chelation.
ToxDetox could be a good choice since EDTA removes iron first and other metals (mercury, lead, cadmium) later due to the affinity list of EDTA.
High intake of dietary iron and high iron level in the body are associated with an increased risk for cancer.
A Swiss chelation study resulted in a 90% reduction of cancer mortality over 18 years, indicating yet again a link between high metal (incl. iron) load and a long list of medical conditions.
Unfortunately, it seems that chelation remains a ‘best kept secret’.
What is EDTA please ?
What about the cast iron pans, the non stick alternative to teflon?
Well seasoned cast iron pans used with an extraction fan to pull out the fumes are fine–I use cast iron myself.
Best,
Sally
Are the cast iron lodge pans giving off iron oxide then? What can I switch to using instead?
Yes, I would also like to know about cast iron pans, and what the recommendations for cookware by WAPF are.
Also, for children today who may not have had great prenatal nutrition… Are there steps to reverse some of the issue so they can grow up to be healthy? And no to the TB vax?
I heat my house with an iron wood burning stove, have cast iron pots and live in mine country with lots of iron oxide in waterways….I am very interested in learning more about the potential dangers of iron, and any relevant works sited, thank you so much.
Was also going to request a post on the best cookware, if this is the case! I use enameled cast iron from le creuset and have really grown to love it. It seems like every type of cookware has some possible downsides to it. I’ve heard that clay leaches lead, stainless steel leaches nickel, aluminum is toxic, and now this with cast iron. My grandparents and great grandparents grew up in homes heated exclusively by cast iron stoves, cooked with cast iron and had no breathing problems. My great grandpa still lives in the home he was born at, wood stove and wood furnace, both iron, no breathing problems. Maybe it’s a ventilation issue? It seems like there could be industrial pollution reasons too. Either way, I’m grateful that you are talking about it if you noticed a pattern! We will never find the best cooking method if everything isn’t considered.
Well seasoned cast iron pans used with an extraction fan to pull out the fumes are fine–I use cast iron myself.
Best,
Sally
In Europe, the old cast iron wood stoves have become a VERY treasured item with this energy crisis and oncoming winter. It will be interesting to look at data of TB increasing???
I love my cast iron 12 1/2″ inch fry pan, purchased in the late 70’s, $8.00. At a gas station that sold some camping supplies. Still looks like new. Every few times I use it, I put some shortening or oil in and put it on the stove over low heat for about 30 minutes. We used it when camping over an open flame, stove top cooking. Never soak in water for extended times, Had to stop for a while when my husband was diagnosed with high iron levels, ran in his family. So then I used it only occasionally. Levels normalized again. I did purchase a small Lodge cast iron pan. Not the same quality. I got rid of it. I’m sure if you looked around you could find one of higher quality. I just made chicken pieces in it, seasoned, oiled, 450 degrees, heated pan before adding oil and chicken, 15min. on each side. 30 minutes total, delicious, tender. temp should be 165 for safe eating. I checked to see if there was a brand name on the bottom, there wasn’t. just No. 10, 12 7/12 inch, 5-1. If you have elevated iron levels you shouldn’t use cast iron. We purchased some stainless steel cookware, safe. do have a 12″ non stick fry pan for eggs and such, but you want to be sure there is no aluminum or other harmful chemicals.